Why in the News?
In the landmark judgment of Harish Rana v. Union of India & Ors (2026), the Supreme Court, for the first time, permitted withdrawal of life-supporting care for a man who has been in a vegetative state for the past 13 years.
Key Highlights of Judgement
- SC waived the usual 30-day consideration period as the patient's parents and medical boards unanimously agreed that recovery was impossible.
- The judgment is governed by the best interests of the patient principle.
- SC ruled that Clinically Assisted Nutrition and Hydration (CANH) is a medical treatment that may be lawfully withdrawn if it serves no therapeutic purpose and only prolongs a vegetative state.
About Passive Euthanasia
- Euthanasia refers to the hastening of a patient's death to relieve suffering. It is broadly classified into two types, i.e. Active and Passive Euthanasia.
- Active euthanasia is the deliberate, direct act of causing a patient's death to end suffering, usually by administering lethal medication.
- It is illegal in India but legal in countries such as the Netherlands, Belgium, Canada, Australia, etc.
- Active euthanasia is the deliberate, direct act of causing a patient's death to end suffering, usually by administering lethal medication.
- Passive euthanasia means allowing a person to die naturally by withholding life-sustaining treatment such as cardio-pulmonary resuscitation, ventilator support, specialised nutrition, etc.
- Passive euthanasia is further classified as voluntary and non-voluntary.
- Voluntary euthanasia is where consent is taken from the patient.
- In non- voluntary euthanasia, consent is unavailable on account of the condition of the patient (E.g. Harish Rana case, 2026).
Legal Status of Passive euthanasia
- Maruti Shripati Dubal v. State of Maharashtra (1987): The court said that the right to die is part of the right to live under Article 21 and said that Section 309 IPC (related to suicide) is not constitutional.
- It was changed in Gian Kaur v. State of Punjab (1996) by the Supreme Court.
- SC said that Section 309 IPC is constitutional and the right to life includes the right to live with dignity, but not to die too soon
- It was changed in Gian Kaur v. State of Punjab (1996) by the Supreme Court.
- Aruna Ramchandra Shanbaug case (2011): SC rejected a plea for euthanasia, but allowed passive euthanasia under strict conditions for terminal and irreversible patients.
- In Common Cause Judgment (2018): SC recognised it and held that the right to die with dignity is a fundamental right under Article 21.
- In this case, it laid down guidelines for it and recognised the concept of a 'living will', with oversight involving DMs, judicial officers and medical specialists.
- A living will refers to a written document that a person uses to give his explicit instructions in advance about medical treatment to be administered if he becomes incompetent or is unable to communicate.
- In this case, it laid down guidelines for it and recognised the concept of a 'living will', with oversight involving DMs, judicial officers and medical specialists.
- Modified Guidelines issued by the SC in 2023
Arguments in favour of Passive Euthanasia
- Patient Autonomy: It upholds the patient's right to make decisions about their own life and death and upholds their right to die with dignity, as upheld by the SC in Common Cause vs. Union of India (2018) case.
- Ensures Dignified Death: It prevents prolonged artificial survival in a vegetative or terminal state through life-sustaining treatment, aligning with humane values.
- Reduces Suffering: It can avoid unnecessary pain caused by treatment like chemotherapy in terminal illnesses like end-stage cancer, and is supported by the ethical principle of beneficence (acting in the patient's best interest).
- Reduced burden: It alleviates the emotional and financial burdens of prolonged life-sustaining treatments such as ventilators, ICUs, etc.
- Legal Clarity: Judicial recognition along with clear guidelines on Passive Euthanasia provides a structured framework (medical boards, consent procedures), reducing ambiguity for doctors and families.
Arguments against Passive Euthanasia
- Misuse and Coercion: There is a risk that family members may unduly influence decisions for inheritance, financial relief, or reducing caregiving responsibilities, thereby exposing vulnerable groups (elderly, disabled etc.) to exploitation.
- Sanctity of Life vs. Autonomy: Many moral and religious traditions consider life sacred and oppose any form of hastening death, which can create tension between individual rights and societal ethical values.
- Weak Institutional Safeguards: Implementation challenges such as lack of awareness about living wills, limited ethics committees etc. may lead to risk of procedural lapses.
- Diagnostic and Prognostic Uncertainty: Medical science is not infallible, and cases of unexpected recovery exist. An incorrect prognosis may result in irreversible and premature end-of-life.
- Non-maleficence: Principle of non-maleficence (do no harm), aligned with Hippocratic Oath—emphasizes that medical professionals must not cause harm to patients.
Way ahead
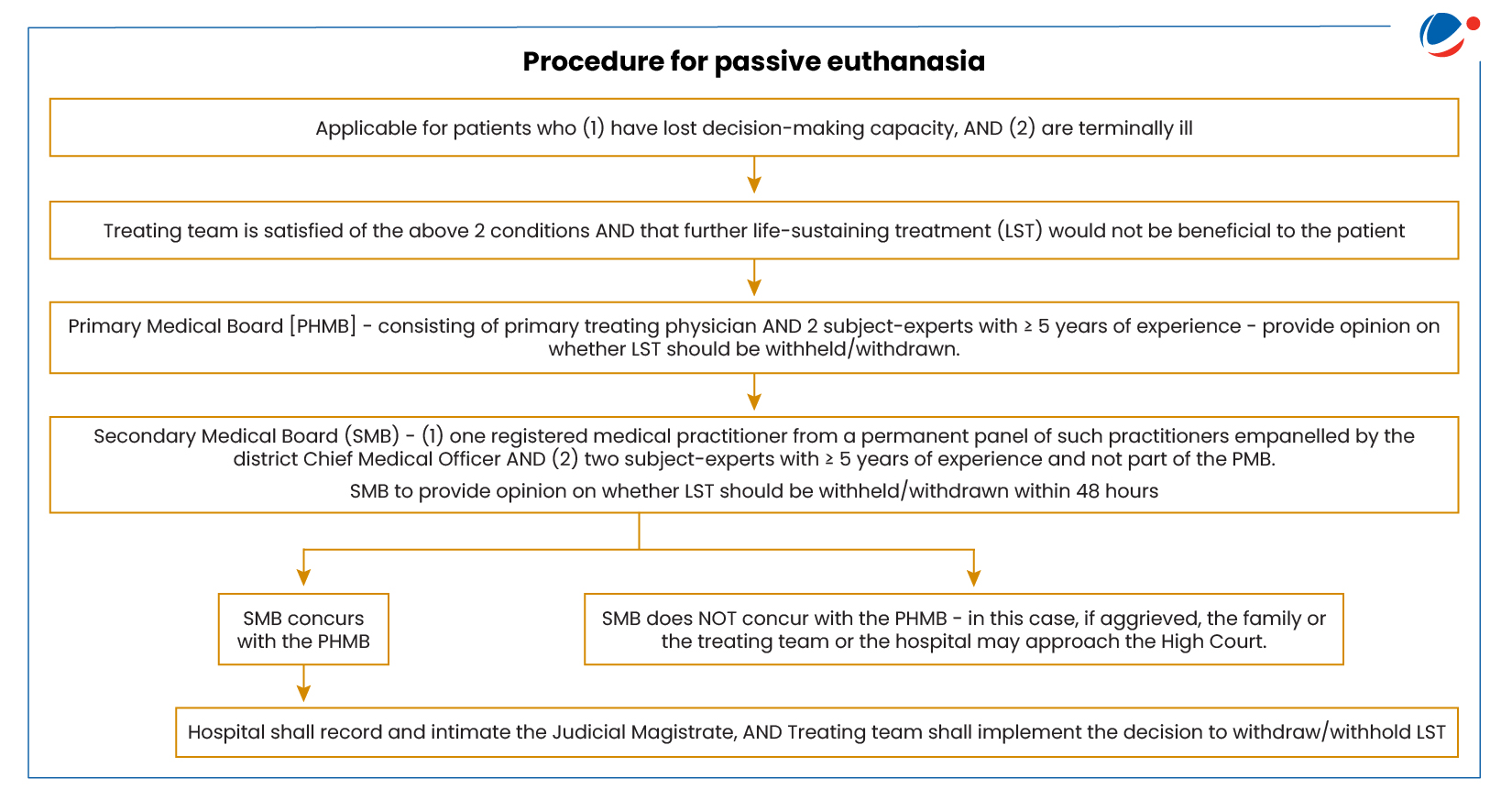
- Multi-Tier Medical Decision Framework: Institutionalisation of Primary and Secondary Medical Boards to ensure independent, expert-driven, and objective assessment of the patient's condition.
- Application of 'Best Interest of Patient' Principle: Decisions must holistically evaluate medical factors (irreversibility, futility of treatment) along with non-medical aspects (dignity, suffering, wishes of caregivers) to ensure ethically sound outcomes.
- Defined Role of State and Administrative Machinery: Governments should facilitate the implementation of Common Cause Guidelines more effectively through:
- Nominate officials in local government as the Custodianship of Living Will.
- Clear directions for the constitution of medical boards to hospitals.
- Empowering CMOs to nominate competent medical practitioners.
- Oversight and Review Mechanisms: Provision for reconsideration periods, supervisory judicial intervention (in case of disagreement), and institutional checkpoints to prevent misuse and ensure procedural fairness.
- Promotion of Palliative Care: Withdrawal of treatment should not mean abandonment but a shift to supervised palliative and end-of-life (EOL) care that relieves pain, manages symptoms, and preserves dignity with minimal suffering.
- Legislative Backing: SC urged the Central Government to consider enacting a comprehensive legislation on EOL care and passive euthanasia, which can be considered.

